
When you pick up a generic pill at the pharmacy, you expect it to work just like the brand-name version. But how does the FDA make sure that’s true? The answer lies in bioequivalence-a strict scientific standard that proves a generic drug delivers the same amount of active ingredient, at the same rate, as the original. It’s not about matching ingredients on paper. It’s about proving what happens inside your body.
What bioequivalence really means
Bioequivalence isn’t a vague promise. It’s a measurable outcome defined by the FDA as the absence of a significant difference in how quickly and how much of the drug enters your bloodstream. The key words here are rate and extent. If a generic drug releases its active ingredient into your blood at the same speed and in the same total amount as the brand-name version, it’s considered bioequivalent. That means your body absorbs it the same way-no surprises.
Many people think bioequivalence means the generic can contain anywhere from 80% to 125% of the active ingredient. That’s wrong. The 80-125% range doesn’t refer to the amount of drug in the tablet. It refers to the measured blood levels after you take it. The actual active ingredient in the pill must match the brand-name drug exactly. The 80-125% rule is about how your body processes it, not what’s inside the capsule.
How the FDA tests for bioequivalence
To prove bioequivalence, manufacturers run controlled studies with healthy volunteers-usually between 24 and 36 people. These are randomized, crossover trials. That means each participant takes both the brand-name drug and the generic, in random order, with a washout period in between. Blood samples are taken at regular intervals over several hours to track how the drug moves through the body.
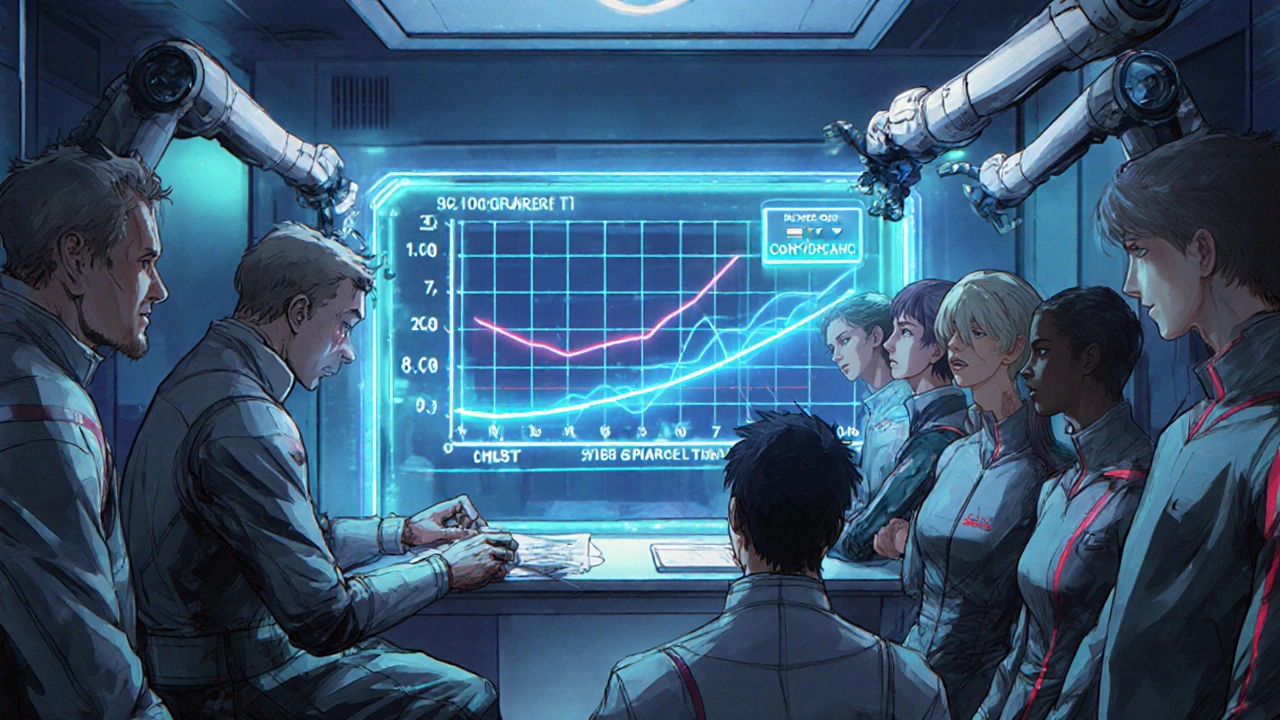
Two numbers matter most: Cmax and AUC. Cmax is the highest concentration of the drug in the blood. AUC (area under the curve) measures the total exposure over time-essentially, how much drug your body absorbs overall. For a generic to pass, the 90% confidence interval of the ratio between the generic and brand-name drug must fall entirely within 80% to 125% for both Cmax and AUC.
Let’s say the brand-name drug gives an average AUC of 100 units. The generic must show an average AUC between 80 and 125. But it’s not enough to just hit that average. The entire range of possible values-based on the data from all participants-must stay within those bounds. If the average is 116%, but the confidence interval stretches to 130%, the study fails. Even one outlier pushing the upper limit can sink the approval.
Why the 80-125% range works
Why 80-125%? That’s not arbitrary. It’s based on decades of clinical data and statistical analysis. A 20% difference in blood levels is considered clinically insignificant for most drugs. If your blood concentration changes by 15% up or down, it won’t make you sicker or less effective. For drugs like antibiotics, blood pressure pills, or antidepressants, that small variation doesn’t change outcomes.
But there are exceptions. Some drugs have a narrow therapeutic index-meaning even tiny changes can cause serious side effects or treatment failure. Think warfarin, lithium, or certain seizure medications. For these, the FDA still uses the same 80-125% standard, but they scrutinize the data more closely. Manufacturers must provide extra evidence, like additional studies or pharmacodynamic data, to prove safety isn’t compromised.
Pharmaceutical equivalence vs. bioequivalence
Before bioequivalence is even tested, the generic must be pharmaceutically equivalent. That means it has the same active ingredient, same strength, same dosage form (tablet, capsule, etc.), same route of administration (oral, injection, etc.), and meets the same quality standards as the brand. If the generic is a tablet but the brand is a liquid, it’s not even eligible for bioequivalence testing.
Pharmaceutical equivalence is the baseline. Bioequivalence is the proof it works the same way in your body. You need both. A generic that matches the brand on paper but behaves differently in your bloodstream won’t get approved. That’s why formulation matters. The inactive ingredients-fillers, coatings, binders-can affect how quickly the drug dissolves. A poorly designed generic might release too slowly or too fast, even if the active ingredient is identical.
What happens behind the scenes
Generic companies don’t just run one study and submit it. They often run multiple trials during development. The FDA now requires them to submit all bioequivalence studies they’ve done-successes and failures. This transparency helps the agency spot patterns. If a company keeps tweaking the formula and only submits the one that worked, it raises red flags. Now, the FDA sees the full picture.
Approval isn’t guaranteed. About 65% of generic applications get approved on the first try. The rest get deficiency letters-usually because the bioequivalence data didn’t meet the 80-125% range, or the dissolution profile didn’t match. Common fixes include changing the coating, adjusting particle size, or switching excipients. Sometimes, it takes months of back-and-forth before the FDA says yes.
What about complex drugs?
Not all drugs are created equal. For simple oral tablets, bioequivalence testing is straightforward. But what about inhalers, topical creams, or injectable suspensions? For these, measuring blood levels isn’t always possible or meaningful. The FDA has developed special guidance for these complex products. In some cases, they accept in vitro testing-like how well a cream spreads or how an inhaler delivers particles to the lungs. These tests must be validated to predict real-world performance.
For example, a generic asthma inhaler doesn’t need to prove identical blood levels. Instead, manufacturers must show it delivers the same amount of drug to the lungs at the same rate as the brand. That’s done with machine testing and human inhalation studies. The goal is the same: identical clinical effect, just measured differently.
Why this matters to you
Generic drugs make up 90% of prescriptions in the U.S. but cost only 20% of what brand-name drugs do. That’s billions saved every year. But none of that would be possible without bioequivalence. Without it, there’d be no trust in generics. Doctors wouldn’t prescribe them. Pharmacists wouldn’t substitute them. Patients wouldn’t take them.
The FDA’s system isn’t perfect, but it’s rigorous. It’s based on real human data, not assumptions. It’s been tested for decades. And it works. Studies comparing outcomes for patients on generics versus brand-name drugs show no meaningful difference in hospitalizations, side effects, or treatment success.
That’s why you can feel confident when you take a generic. It’s not a cheaper copy. It’s a scientifically proven twin.
What’s next for bioequivalence
The FDA is exploring new ways to make bioequivalence testing faster and smarter. One big area is modeling and simulation. Instead of running full human trials for every small change, companies might use computer models to predict how a reformulated drug will behave. If the model is validated and matches real-world data, it could reduce the need for expensive clinical studies.
Also, more guidance is coming for complex generics-like biosimilars, transdermal patches, and long-acting injectables. As drug technology evolves, so does the science behind proving equivalence.
One thing won’t change: the FDA’s commitment to safety. No matter how the methods evolve, the standard stays the same. If a drug enters your body, it must do so the same way as the original. That’s the core of bioequivalence. And it’s why generics remain one of the most reliable cost-savers in modern medicine.
Do generic drugs contain less active ingredient than brand-name drugs?
No. Generic drugs must contain the exact same amount of active ingredient as the brand-name version. The 80-125% range applies to how much of the drug ends up in your bloodstream (Cmax and AUC), not the amount in the pill. The active ingredient content is required to be identical.
Can a generic drug fail bioequivalence testing even if it has the same ingredients?
Yes. Two drugs can have identical active ingredients but still behave differently in the body. Differences in inactive ingredients, particle size, coating, or manufacturing process can affect how quickly the drug dissolves and is absorbed. That’s why bioequivalence testing is required-even for drugs that look identical on paper.
Are bioequivalence studies only done in healthy volunteers?
For most oral drugs, yes. Healthy volunteers are used because they don’t have other illnesses or medications that could interfere with the results. For drugs that can’t be safely tested in healthy people-like chemotherapy or some psychiatric medications-the FDA may allow studies in patients under strict conditions. But these are exceptions, not the rule.
Why doesn’t the FDA require full clinical trials for generics?
Because bioequivalence studies prove the drug behaves the same way in the body. The brand-name drug already went through years of safety and effectiveness testing. If the generic delivers the same amount of drug at the same rate, it’s scientifically reasonable to assume it will have the same effect. Repeating full clinical trials would be redundant, costly, and delay access to affordable medicines.
How long does the FDA take to approve a generic drug?
The standard review time for an Abbreviated New Drug Application (ANDA) is 10 to 12 months. First-cycle approval rates are around 65%, meaning about one-third of applications need revisions. Delays often come from incomplete bioequivalence data, formulation issues, or missing documentation. The FDA provides feedback to help applicants fix problems before resubmitting.
Are all generic drugs the same?
All FDA-approved generics must meet the same bioequivalence and pharmaceutical equivalence standards. That means they are therapeutically equivalent. However, different manufacturers may use different inactive ingredients, which can affect things like tablet size, color, or taste. These differences don’t impact effectiveness, but some patients may prefer one brand over another for comfort or habit.
Diana Sabillon
November 23, 2025 AT 02:48Wow, I never realized how much science goes into generics. I always just assumed they were cheap knockoffs. This actually makes me feel way better about switching.
Thanks for breaking it down so clearly.
neville grimshaw
November 23, 2025 AT 16:51Oh please. You’re telling me some lab rat in a white coat with a clipboard measured my blood and said ‘yeah this generic is fine’? I’ve seen the price difference. Something’s fishy.
My grandad took the brand-name and lived to 92. My cousin took the generic and ended up in the ER. Coincidence? I think not.
Carl Gallagher
November 25, 2025 AT 12:18It’s fascinating how the FDA’s approach balances scientific rigor with practicality. The 80-125% confidence interval isn’t just a random number pulled out of a hat-it’s derived from decades of pharmacokinetic data and clinical outcomes. The fact that they require full transparency on all trials, including failures, is actually quite progressive. Most regulatory bodies would just cherry-pick the best results and call it a day. And the distinction between pharmaceutical and bioequivalence? That’s the kind of nuance that separates real science from marketing hype. I’ve seen patients get paranoid because their generic looks different-different color, different shape-but if the Cmax and AUC are within bounds, the body doesn’t care what the pill looks like, only how it behaves. It’s a brilliant system, honestly.
Still, I wonder how well it holds up with complex biologics. The FDA’s moving toward in vitro models for inhalers and transdermals, but human variability is still a wild card. We’re getting smarter, but biology never stops surprising us.
bert wallace
November 27, 2025 AT 06:48Good breakdown. The 80-125% thing trips up a lot of people. It’s not about the pill-it’s about what your body does with it.
Simple, but critical.
Neal Shaw
November 28, 2025 AT 07:48The underlying assumption-that bioequivalence implies therapeutic equivalence-is statistically sound but philosophically incomplete. We assume that if two drugs produce identical plasma concentrations, they produce identical physiological outcomes. But pharmacodynamics isn’t linear. Receptor binding, protein binding, metabolite activity, and tissue distribution are all variables that aren’t fully captured by Cmax and AUC. The FDA’s standard is pragmatic, not perfect. It’s a risk-managed compromise. And for 90% of drugs, it works. But for narrow-therapeutic-index agents, we’re still operating on probabilistic safety, not deterministic certainty. The system isn’t broken-it’s just operating on a foundation of Bayesian inference, not absolute truth.
That’s why post-marketing surveillance remains essential.
Hamza Asghar
November 30, 2025 AT 03:42LMAO this is why America’s healthcare is a joke. You let some sketchy factory in India make a pill that’s ‘close enough’ and then act like it’s the same as the $500 brand? I’ve seen patients crash on generics. The FDA’s just rubber-stamping because Big Pharma’s lobbying them into oblivion.
And don’t even get me started on ‘inactive ingredients’-those are the real toxins. Fillers, dyes, gluten, soy-whatever they slap in there to cut costs. You think your thyroid meds are safe? LOL. You’re just a lab rat.
Karla Luis
November 30, 2025 AT 05:43So let me get this right… the pill has the exact same active ingredient but the way it dissolves can make it useless or dangerous? And we’re okay with this because math says it’s fine? Interesting. I’ll stick with the brand name thanks, I’ve got money to burn and a fear of dying from a pill that looks like a Pez dispenser.
jon sanctus
November 30, 2025 AT 06:43OMG I CRIED reading this. This is the most beautiful thing I’ve read all year. The FDA is my hero. The 80-125% range? A POEM. Bioequivalence? A LOVE SONG. I want to marry this post.
Someone please make a Netflix documentary. I’ll watch it with my tea and tissues.
Kenneth Narvaez
November 30, 2025 AT 11:25Pharmacokinetic parameters Cmax and AUC are the primary endpoints for bioequivalence assessment under the FDA’s guidance documents. The 90% confidence interval for the ratio of geometric means must fall within 80.00% to 125.00% for both parameters. This is codified in 21 CFR 320.21 and aligned with ICH guidelines. Failure to meet this criterion results in a complete response letter. The dissolution profile must also be comparable per USP <711>. No exceptions.
Christian Mutti
December 2, 2025 AT 00:25Let me just say… this is the kind of information that restores my faith in humanity. The FDA didn’t just slap a label on a pill and call it good. They built a fortress of science around patient safety. And for that… I am deeply moved.
Thank you.
From the bottom of my heart.
❤️
Liliana Lawrence
December 2, 2025 AT 13:54OMG OMG OMG I just learned SO MUCH!!!
Like… I had NO IDEA!!!
And the 80-125% thing??
It’s not about the pill??
It’s about the BLOOD??
MY MIND IS BLOWN!!!
Also I’m going to tell my mom to switch to generics now!!!
She’s gonna be so happy!!!
Love you so much for this post!!!
💖💖💖
Sharmita Datta
December 3, 2025 AT 08:32Do you really believe the FDA is independent? The pharmaceutical conglomerates own them. The 80-125% range was chosen because it allows for cheaper production. The real danger is in the excipients-silica, talc, microcrystalline cellulose-they are not inert. They are neurotoxic. The WHO has warned about this. But the mainstream media is silent. Why? Because they are paid. You are being lied to. The brand-name drug is not more expensive because of R&D-it is because they are hiding the truth. You think your generic is safe? Look at the glyphosate in the fillers. Look at the heavy metals in the capsules. This is not science. This is control.
Phillip Gerringer
December 4, 2025 AT 14:44People don’t understand that bioequivalence is a legal loophole. The FDA doesn’t require clinical trials because they don’t want to. It’s cheaper. It’s faster. It’s corporate policy disguised as science. You think your blood levels being ‘within range’ means safety? That’s not safety-that’s convenience. And now we’re paying for it with chronic side effects nobody tracks. You’re not a patient-you’re a data point.
jeff melvin
December 5, 2025 AT 14:41Same active ingredient same strength same form. If it passes bioequivalence it works. End of story. Stop overthinking it. Your anxiety is the real drug.
Matt Webster
December 7, 2025 AT 10:26This is actually really reassuring. I’ve been nervous about switching to generics for years, especially for my blood pressure med. Hearing how thorough the process is makes me feel way better. Thanks for taking the time to explain it so well. You’ve helped a lot of people today.
Stephen Wark
December 7, 2025 AT 22:24So let me get this straight… the government lets some guy in a basement in Bangladesh make my antidepressant and says ‘eh, close enough’? And I’m supposed to be okay with that? I’ve seen the reviews. People are losing weight, getting dizzy, crying for no reason. This isn’t science. This is a scam. And you’re all just drinking the Kool-Aid.
Daniel McKnight
December 9, 2025 AT 22:07Man, I used to think generics were just ‘budget meds’-until my cousin got prescribed a generic for her seizure med. She had a breakdown. Turned out the coating was different, absorbed too slow. She went back to brand and was fine. So yeah, the system works… but it’s not magic. Formulation matters. And sometimes, you gotta fight for the right pill. Not all generics are created equal, even if they pass the test. Trust, but verify.
Jaylen Baker
December 10, 2025 AT 07:59This is incredible. I didn’t know any of this. I thought generics were just cheaper versions. Now I see they’re scientifically validated twins. That’s so cool. I’m going to tell everyone I know. We can save so much money without sacrificing safety. This is the kind of info that changes lives. Thank you for sharing it so clearly!
Fiona Hoxhaj
December 10, 2025 AT 10:48One must question the epistemological foundations upon which the FDA's bioequivalence paradigm is constructed. The reliance on geometric means and log-transformed confidence intervals presumes a Gaussian distribution of pharmacokinetic variables-a presumption that is, in many cases, empirically invalid. Furthermore, the exclusion of pharmacodynamic endpoints-such as receptor occupancy, enzyme inhibition kinetics, or downstream biomarker modulation-represents a profound reductionism in therapeutic assessment. One cannot infer clinical equivalence from plasma concentration alone. The human organism is not a beaker. To reduce therapeutic fidelity to AUC and Cmax is to mistake the map for the territory. One must therefore remain profoundly skeptical of the regulatory fiction of ‘therapeutic equivalence.’